Respiratory Depression from Opioids and Other Medications: Critical Signs You Can't Ignore
Feb, 7 2026
Respiratory Depression Risk Calculator
Assess Your Risk
Risk Assessment Results
Enter your information to see your risk level
Critical Signs to Watch For
When someone takes an opioid - whether it's oxycodone after surgery, fentanyl for chronic pain, or even a prescription painkiller they got from a friend - their body doesn't just feel less pain. It also starts to slow down one of the most basic, life-sustaining functions: breathing. This isn't a rare side effect. It's a dangerous, predictable, and often preventable reaction called opioid-induced respiratory depression (a condition where the brain's control over breathing weakens due to opioid action on the brainstem). And left unchecked, it can kill someone in minutes.
What Does Respiratory Depression Actually Look Like?
It doesn’t always start with someone turning blue or collapsing. Early signs are quiet. Subtle. Easy to miss.
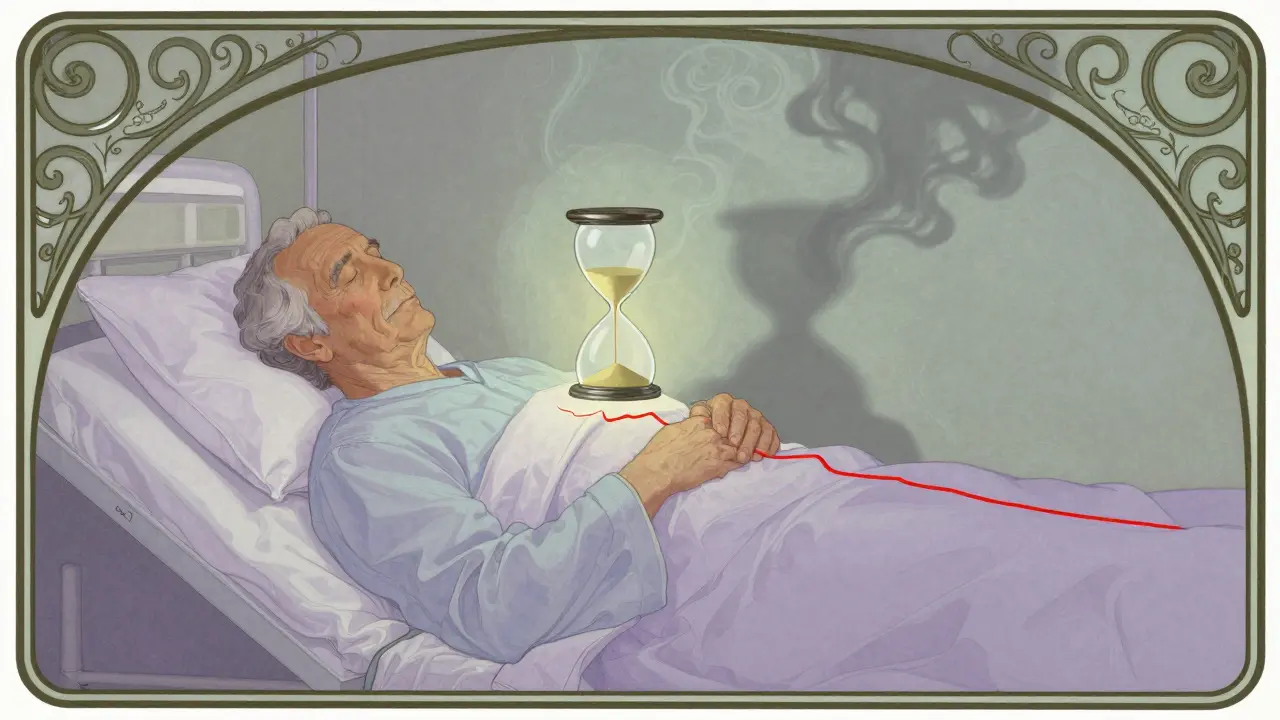
Think about this: a patient in a hospital room after surgery is resting. Their oxygen level reads 96% on the monitor. They look calm. But their breathing? Only 7 breaths per minute. That’s below the danger threshold of 8-10 breaths per minute. Their body is holding onto oxygen thanks to supplemental oxygen, but carbon dioxide is building up silently in their blood. That’s the real danger - hypercapnia. And it’s not visible.
The classic signs (a cluster of symptoms indicating central nervous system depression from opioids) include:
- Shallow, slow, or irregular breathing - fewer than 8 breaths per minute
- Low oxygen saturation (below 85%) - especially if not on supplemental oxygen
- Extreme drowsiness or inability to wake up, even when shaken
- Confusion or disorientation - they don’t know where they are or who you are
- Bluish lips or fingertips - a late sign, meaning oxygen is already critically low
- Slow heart rate (bradycardia) - though some patients show fast heart rate instead
Here’s what’s scary: supplemental oxygen (can mask the early warning of low oxygen, while carbon dioxide rises unnoticed). A patient on oxygen might have a normal pulse ox reading but still be in respiratory arrest. That’s why pulse oximetry alone isn’t enough.
It’s Not Just Opioids - Other Drugs Make It Worse
Most people think respiratory depression only happens with heroin or prescription painkillers. But it’s not that simple.
Drugs like benzodiazepines (including diazepam, alprazolam, and lorazepam - used for anxiety or sleep), alcohol (a central nervous system depressant that amplifies opioid effects), sleep aids (such as zolpidem or zaleplon), and even some muscle relaxants can team up with opioids to shut down breathing.
When opioids are combined with benzodiazepines, the risk of respiratory depression jumps 14.7 times (based on clinical data from the Cleveland Clinic). That’s not a small increase. That’s a catastrophic one.
And it’s not just about street drugs. A 72-year-old woman on oxycodone for back pain who also takes lorazepam for anxiety? She’s in the danger zone. A 45-year-old man on tramadol after a knee surgery who has a glass of wine with dinner? He’s at risk.
Who’s Most at Risk?
Not everyone who takes opioids develops respiratory depression. But some people are sitting on a ticking clock.
Research shows these factors dramatically increase risk:
- Age over 60 - risk increases 3.2 times
- Female sex - 1.7 times higher risk than males
- Opioid-naïve patients - those who’ve never taken opioids before - 4.5 times more likely to develop depression
- Multiple health conditions - each additional condition (like COPD, heart failure, or sleep apnea) raises risk by 2.8 times
- Using more than one CNS depressant - the combination is deadly
And here’s the brutal truth: most patients aren’t monitored closely enough (a 2023 study found patients checked every 4 hours are unmonitored 96% of the time). That means someone could start slowing down at 2 a.m. and not be noticed until 6 a.m. - by then, it’s often too late.
How Hospitals Are Trying to Stop It
Some places are fighting back - and winning.
Leading hospitals have cut respiratory depression cases by 47% using just three strategies:
- Continuous monitoring - using capnography (which measures carbon dioxide) for patients on oxygen, and pulse oximetry for those who aren’t. Alarms set at respiratory rate below 10 or oxygen saturation below 90%.
- Pharmacist-led dosing - pharmacists review opioid prescriptions for high-risk patients and adjust doses based on individual risk factors.
- Staff training - every nurse, aide, and tech learns to recognize the early signs, not just wait for alarms.
But most hospitals aren’t doing this. Only 22% of U.S. hospitals meet all the safety standards recommended by the Anesthesia Patient Safety Foundation. Community hospitals? Only 14% do.
And alarm fatigue is real. Nurses hear so many false alarms that they start ignoring them. That’s why smart systems are being developed - ones that predict respiratory depression 15 minutes before it happens, using trends in breathing rate, heart rate, and movement.
What Happens If It’s Not Caught?
Without intervention, respiratory depression leads to:
- Severe carbon dioxide buildup - which poisons the brain
- Oxygen starvation - causing brain damage in as little as 3-5 minutes
- Cardiac arrest - from lack of oxygen
- Death
And here’s the kicker: it’s preventable. This isn’t a medical mystery. We know how to stop it. But we’re not doing it consistently.

What Should You Do?
If you or someone you care for is on opioids:
- Never mix opioids with alcohol, benzodiazepines, or sleep meds - even one drink can be dangerous.
- Ask about risk assessment - hospitals should screen for age, sex, comorbidities, and medication use before giving opioids.
- Request continuous monitoring - especially if the patient is elderly, opioid-naïve, or on multiple drugs.
- Know the signs - if someone can’t be woken up, or is breathing less than 8 times a minute, call for help immediately.
- Have naloxone on hand - it reverses opioid effects. Keep it in your medicine cabinet if someone at home takes opioids. Train family members how to use it.
And if you’re a caregiver or family member - don’t assume the hospital is watching. Ask: “Are they being monitored continuously?” If the answer is no, push for it.
The Bottom Line
Respiratory depression from opioids isn’t an accident. It’s a failure of vigilance. We have the tools. We have the knowledge. We have the technology. But we’re still letting people slip through the cracks.
It doesn’t have to be this way. With better monitoring, smarter dosing, and trained staff - these deaths can be stopped. Before they even start.
Can you die from respiratory depression even if you're on oxygen?
Yes. Supplemental oxygen keeps oxygen levels high, but it doesn’t stop carbon dioxide from building up. When breathing slows too much, CO2 rises to toxic levels - this is called hypercapnia. The brain can’t sense this without proper monitoring, and it can lead to unconsciousness, cardiac arrest, or death - even if the pulse oximeter shows 95%.
How quickly can opioid-induced respiratory depression happen?
It can happen within minutes after an IV dose, especially in opioid-naïve patients. For oral medications, it may take 30-60 minutes to peak. But in high-risk patients, even a single dose can trigger a slow decline over hours. That’s why monitoring for at least 2 hours after dosing is critical.
Is naloxone always the right treatment?
Naloxone is the standard reversal agent, but it must be used carefully. Giving too much too fast can cause sudden opioid withdrawal - leading to agitation, high blood pressure, and even heart rhythm problems. In chronic pain patients, it can also remove pain relief. The goal is to restore breathing without triggering withdrawal - often requiring small, repeated doses.
Why aren’t all hospitals using capnography?
Cost, staffing, and lack of policy. Capnography devices are more expensive than pulse oximeters, and many hospitals don’t have enough trained staff to interpret the data. Some still rely on outdated practices like checking vitals every 4 hours. But studies show capnography catches 94% of respiratory events when oxygen is used - making it the gold standard for high-risk patients.
Can you build tolerance to respiratory depression?
You can develop tolerance to the pain-relieving effects of opioids, but not fully to respiratory depression. That’s why people who’ve been on opioids for years can still overdose - especially if they take more than usual, or combine it with other depressants. The body doesn’t learn to breathe better - it just learns to tolerate more pain.








